Capnography
What does this channel measure?
This channel measures the partial pressure of carbon dioxide (CO2) in the subject’s expired air (pCO2).
Especially relevant is the end-tidal value at the end of a complete expiration, which corresponds closely to
arterial values at the arterioles deep inside the lung where gas exchange between outside air and the blood takes place.
End-tidal pCO2 (ETPCO2) is the gold-standard non-invasive measure of hypocapnia (low pCO2) and hypercapnia (high pCO2),
corresponding to hyper- and hypoventilation.
In ANSLAB the capnography analysis starts with displaying the end-tidal pCO2 values over the duration of the file and
the corresponding breathing rates.

Normal healthy baseline values for ETPCO2 are approximately 38 +/- 5 mmHg. Consistently lower values often indicate hyperventilation due to
emotional activation. For editing, you should be mainly concerned with sudden spikes in the data. Slower, relatively consistent trends in the
data are typically due to changes in the breathing pattern producing blood gas changes.
[
Top]
What kind of artifacts are common in this channel?
The most common problem with ETPCO2 measurement is an incomplete exhalation through the nose (where the sampling line is attached),
e.g. due to partial breathing through the mouth, speaking, shallow breathing, or early termination of exhalation.
Many values from instances of these kinds of breaths are automatically excluded by the
program using a strict criterion for a stable end-tidal plateau of expired pCO2. Only values from such plateaus can be assumed to
approximate gas exchange levels at the arterioles. The end-tidal level of a shallow or interrupted expiration will mostly reflect levels of
pCO2 in the dead space or upper parts of the lung. Plateaus from such breaths are typically not flat enough to reach criterion. The same
applies to many end-tidal levels of speech breaths, which are also typically excluded automatically.
However, some of such invalid breaths might not be screened out automatically and will then occur
intermittently in the end-tidal pCO2 display as easily discernible spikes.
But, a prolonged series of very shallow breaths might appear as a rather stable period of low ETPCO2 and needs to be judged in the
context of the results of the respiratory pattern analysis.
[
Top]
How are artifacts removed?
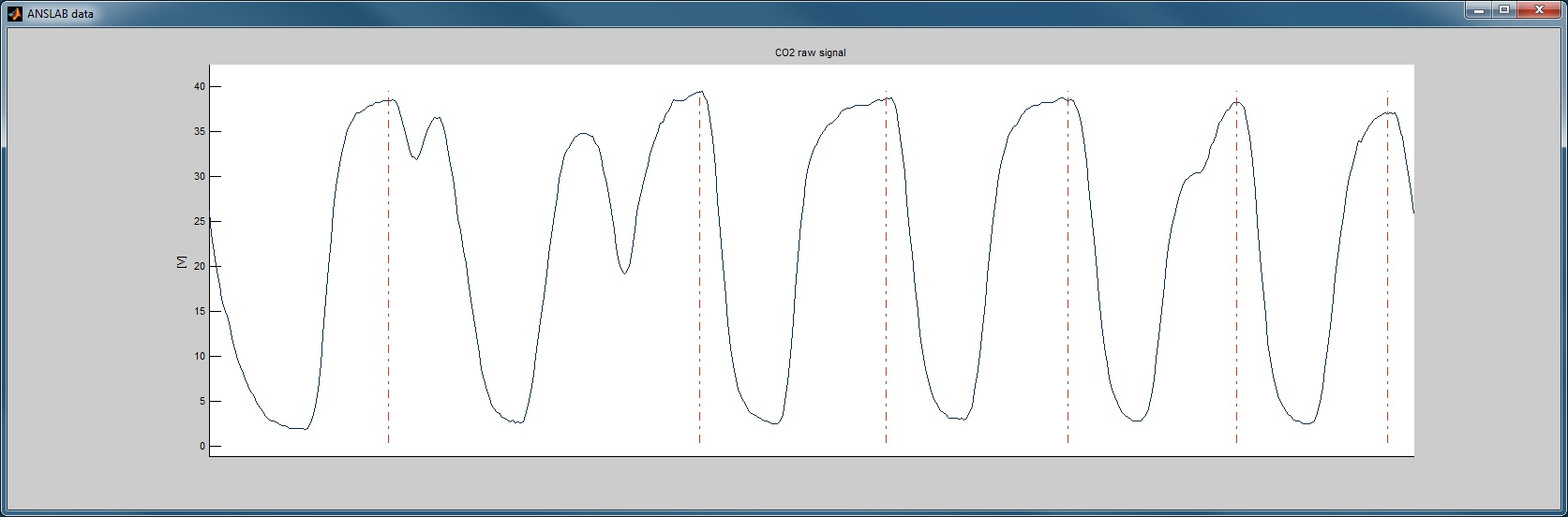
Suspicious intervals should be marked using the 'define segments'-button. After zooming to this interval and
switching to 'raw'-data mode, you can see the raw CO2 signal with vertical red lines indicating points where the end-tidal
plateaus met the stability criterion of the detection algorithm.
You can now either add or delete points using the 'delete' and the 'insert'-button in the
editing section of the ANSLAB command window, or you can move present markers to adjust their position.
Most sudden drops in pCO2 of more than 4 mmHg in one isolated breath without an obvious change in respiratory rate or
pattern preceding or following that breath (e.g. sigh, yawn) are invalid and should be excluded.
[
Top]